Wheels began Speech Therapy at the local regional campus of the State University.
Our first appointments included two students who were co-working because there were not enough clients during Covid. Cozy in a small cubicle with four people! Wheels was interested and attentive, but silent. Compensation was my habit and I couldn’t be quiet. I replied to questions for him, interpreted his gestures and eye movements. It was exhausting and made clear to me how much Wheels had lost.
I brought my little half sheet of information.
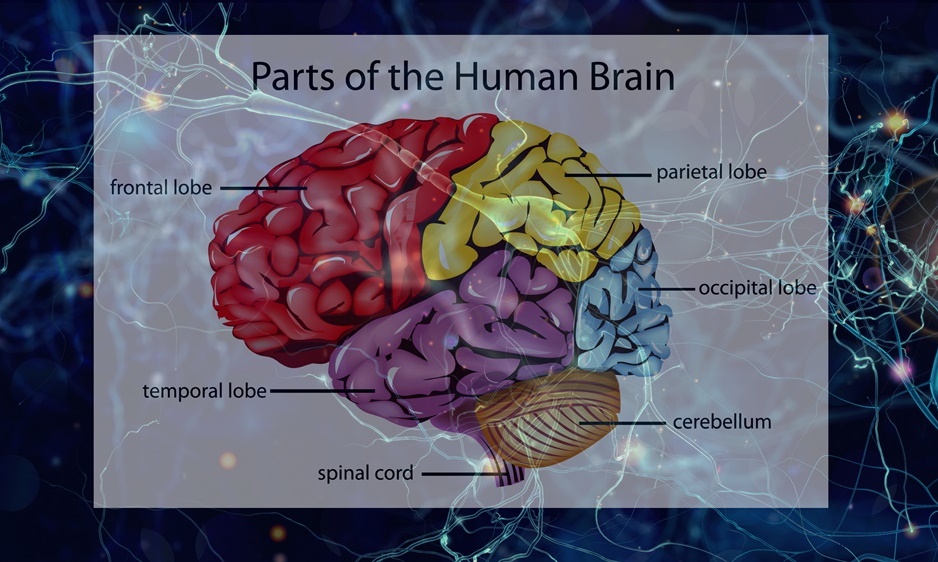
Basically it said: Aphasia is a language disorder often resulting from a stroke or brain injury. Or, as in Wheels’ case, the degeneration of the speech area in the left side of the brain. The left hemisphere controls all aspects of language: comprehension, speaking, reading, and writing. It affects a person’s ability to process, use, and/or understand language. I had compiled a little list of his “quirks”.
The Association for Frontal Temporal Degeneration website, theaftd.org was relatively new at the time of Wheels’ diagnosis. It has exploded in depth of information and visibility. People no longer have to search and carry around a little half page of information like I did. Here is a link to a two page Diagnostic Checklist from their website.
Aphasia does not affect intelligence. Characteristics of the disease vary depending on the location and degree of damage to the brain, and this designates one of the four subtypes of the disease. The greater the severity of the aphasia, the more limited the speech and language skills. The disease is progressive in nature as the brain itself continues to degenerate. There is currently no known cause.
People with nonfluent/agrammatic variant PPA have difficulty speaking but recall word meanings.
The ability to form sounds with their lips and tongue is caused by degeneration of the parts of the brain that control certain related muscles; the muscles themselves, however, are unaffected. The technical term for such problems is apraxia of speech. As a result, speech becomes slow and effortful and patients may appear to be physically struggling to produce words. But speech problems alone are not sufficient for diagnosing PPA. It is the loss of language, that is central to a PPA diagnosis. Language is the structured system of communication used by humans to express thoughts, feelings, and ideas.
Impairment of grammar is the defining feature
People with nfvPPA make many mistakes while speaking, including omitting small grammatical words, using word endings and verb tenses incorrectly, and/or mixing up the order of words in sentences. Eventually, some may develop difficulty swallowing as well as more widespread motor symptoms. . . . This fit Wheel’s speech and behavior exactly, what I thought of as his “quirks”. He lost the ability to walk, then lost the ability to swallow, eventually requiring full care.
We noted “Impaired comprehension of complex sentences” listed as a symptom.
Remember that trip to the dentist office? I said to Wheels as he left for his appointment, “You can do it. It’s easy”. And then I said, “go down to the first corner and turn left until you come to the light, turn right and go up to the next light, don’t turn but go to the next corner, turn right and there is the dentist’s office on the right hand side”. Remember – street names are seldom used in our town. He never had a chance after that speech! Although in my defense, he would have understood before the disease – and grin.
History note:
With the focus on the new developments regarding diagnosis and treatment of FTD, it seems that it is a “new discovery”. Actually it was noted in 1892 by a Czech researcher named Arnold Pick and is still sometimes referred to as Pick’s Disease. Pick published several articles focusing on apraxia, agnosia, memory, consciousness, and psychosis as well as aphasia. It was not until 1920 that Alois Alzheimer had his name attached to a more common brain disease.